Latest News 2026
Research Highlights
JUNE 2026
ERA 2026
Oral presentation: MRA initiation, hyperkalaemia risk and treatment persistence across kidney function groups
The CaRe Study
Presented by Prof. Roberto Pecoits-Filho (Pontifical Catholic University of Paraná, Brazil), this analysis evaluated real-world use of mineralocorticoid receptor antagonists (MRAs) in patients with comorbid heart failure and chronic kidney disease across different levels of kidney function. MRA initiation was associated with only modest average increases in serum potassium, yet hyperkalaemia risk remained high, particularly among patients with impaired kidney function. More than half of patients discontinued treatment within two years, highlighting persistent barriers to durable MRA therapy in routine cardiorenal care. These findings underscore the importance of optimized potassium management strategies to support appropriate and sustained MRA use in high-risk patients.



Presented by prof Roberto Pecoits-Filho, USA at
The 63rd European Renal Association Congress
Glasgow, United Kingdom, June 2026.
JUNE 2026
ERA 2026
Oral presentation: Proteinuria testing patterns in primary care patients with chronic kidney disease: results from England and the USA
The PROMISE Study
Presented by Prof. James Burton (University of Leicester). The PROMISE study demonstrated that proteinuria testing remains markedly underutilized in primary care CKD management, particularly among patients without T2D, potentially limiting timely identification of high-risk patients eligible for guideline-directed cardiorenal-protective therapies.

Presented by prof James O. Burton, UK at
The 63rd European Renal Association Congress
Glasgow, United Kingdom, June 2026.
MAY 2026
ECO 2026
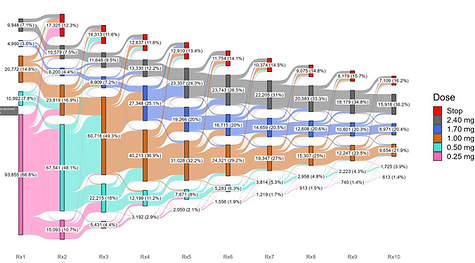
Nationwide analysis of obesity pharmacotherapy reveals individualized real-world use of semaglutide 2.4 mg
Presented by Dr. Jens K. Hertel (Vestfold Hospital Trust, Norway), this nationwide analysis evaluated obesity medication use in more than 140,000 individuals in Norway. The study demonstrated a rapid increase in predominantly self-funded semaglutide 2.4 mg use, which has reshaped the Norwegian obesity treatment landscape. Real-world utilization was characterized by highly individualized dose titration patterns, frequent treatment interruptions and patient-driven dose adjustments ("click-counting"), highlighting important differences between clinical trial protocols and routine clinical practice. These findings demonstrate the value of real-world evidence for understanding the implementation and long-term use of innovative obesity therapies.

Presented Jens K Hertel, Norway, at
The 33rd European Congress on Obesity
Istanbul, Türkiye, May 2026
MAY 2026
ESC HF 2026
Rapid fire presentation: Initiation of MRA in HF and CKD - potassium trajectories, hyperkalaemia and treatment persistence
The CaRe Study
New findings presented by Prof. Stephen Greene (Duke University School of Medicine, Durham, North Carolina, USA) from the CaRe Study demonstrate early and dose-dependent increases in serum potassium following MRA initiation in patients with heart failure and chronic kidney disease. Hyperkalaemia risk increased over time, while treatment persistence declined substantially, with more than half of patients discontinuing treatment within two years. These findings highlight important barriers to sustained MRA use in routine clinical practice and underscore the need for treatment strategies that are both effective and well tolerated in this high-risk population.


Presented prof Stephen Greene at
ESC Heart Failure 2026,
Barcelona, Spain, May 2026
NOVEMBER 2025
ASN
Cardiorenal disease and severe renal outcomes
The CaRe Study
RWE findings presented by Prof. Roberto Pecoits-Filho (Pontifical Catholic University of Paraná, Brazil) from Japan, Sweden and the USA demonstrated that patients with combined chronic kidney disease (CKD) and heart failure face a substantially worse kidney prognosis than those with either condition alone. These findings highlight the considerable burden of cardiorenal disease and underscore the urgent need for improved treatment strategies in this high-risk population.
Presented by prof Roberto Pecoits-Filho, USA at
ASN Kidney Week 2025
Houston, Texas, USA, November 2025.
SEPTEMBER 2025
Adv Ther
UACR 700 mg/g: CKD progression, cardiorenal risk and SGLT2i effects
The OPTIMISE-CKD Study


RWE from the USA shows that patients with CKD and high-risk proteinuria (UACR ≥ 700 mg/g) experience rapid kidney function decline and markedly higher risks of hospitalization and death. Although SGLT2i provide expected benefits, substantial residual albuminuria highlights the urgent need for improved treatment strategies in this high-risk population.
Pecoits-Filho R, Bodegård J, et al. Disease Progression, Clinical Outcomes and Treatment Challenges in Patients with Chronic Kidney Disease and High-Risk Proteinuria. Adv Ther. 2025 Nov;42(11):5653-5668. doi: 10.1007/s12325-025-03364-8. Epub 2025 Sep 15. PMID: 40952621; PMCID: PMC12579703.
AUGUST 2025
ESC 2025
Cardiorenal disease and risks of hospitalizations for HF and CKD
The CaRe Study
RWE findings presented by Prof. Stephen Greene (Duke University School of Medicine, USA) from Japan, Sweden and the USA demonstrated that patients with combined heart failure (HF) and chronic kidney disease (CKD) face substantially higher risks of all-cause mortality and HF- and CKD-related hospitalizations than patients with either condition alone. These findings highlight the severe prognosis associated with cardiorenal disease and underscore the need for integrated management and optimized guideline-directed medical therapy (GDMT) in this high-risk population.
Presented prof Gianluigi Savarese, Sweden at
ESC Congress 2025
Madrid, Spain, August 2025.
AUGUST 2025
ESC 2025
Incident cardiorenal disease and changes in GDMT for HF
The CaRe Study
RWE findings presented by Prof. Gianluigi Savarese (Karolinska Institutet and Södersjukhuset, Stockholm, Sweden) from Japan, Sweden and the USA demonstrated that patients with incident heart failure (HF) and chronic kidney disease (CKD) receive consistently low levels of guideline-directed medical therapy (GDMT), both before and after diagnosis. Despite modest treatment increases following incident HF+CKD, substantial implementation gaps persisted, highlighting the need for earlier identification and optimized management of this high-risk cardiorenal population.
Presented prof Gianluigi Savarese, Sweden at
ESC Congress 2025
Madrid, Spain, August 2025.
JULY 2025
BMC Nephrology
CKD with and without T2D: Risks and GDMT utilization
The OPTIMISE-CKD study
Nationwide RWE from Norway shows that diagnosed CKD is associated with high risks of hospitalization, mortality, and substantial healthcare costs, irrespective of diabetes status. Despite increasing uptake of SGLT2 inhibitors, overall use of kidney-protective therapies remains low—highlighting an urgent need for better GDMT implementation and risk management in CKD.
Jenssen TG, Bodegård J. et al Prevalence, outcomes, costs, and treatments of a contemporary population with chronic kidney disease in Norway: a nationwide observational study. BMC Nephrol. 2025 Jul 17;26(1):393. doi: 10.1186/s12882-025-04171-7. PMID: 40676552; PMCID: PMC12273365.
2 JULY 2025
NICE
Low UACR Restriction for SGLT2i
The OPTIMISE-CKD Study
NICE reversed its prior restriction on dapagliflozin for CKD patients with low UACR (non-T2D, low albuminuria) based on new real-world evidence. This decision reflects growing confidence in high-quality RWE to fill evidence gaps where RCT data are limited.

Svensson MK, Tangri N, Bodegård J, et al Dapagliflozin treatment of patients with chronic kidney disease without diabetes across different albuminuria levels (OPTIMISE-CKD). Clin Kidney J. 2024 Apr 4;17(8):sfae100. doi: 10.1093/ckj/sfae100. PMID: 39165293; PMCID: PMC11333959.
MAY 2025
NDT
CKD stage 3-4 with or without T2D: UACR, risks and GDMT utilization
The OPTIMISE-CKD Study
RWE from Finland shows that stage 3–4 CKD is highly prevalent, with most patients being non-T2D yet experiencing similarly high risks of hospitalization and death. Albuminuria testing and use of kidney-protective therapies were low—especially in non-T2D patients—highlighting an urgent need for improved CKD detection and preventive treatment.
Metsärinne K, Bodegård J, et al. Characteristics, treatment and disease burden among stage 3-4 chronic kidney disease patients with and without type 2 diabetes in Finland during 2016-2022. Nephrol Dial Transplant. 2025 May 30;40(6):1115-1123. doi: 10.1093/ndt/gfae242. PMID: 39510970; PMCID: PMC12209851.
17 MAY 2025
ESC HF 2025
Cardiorenal Disease Pathways
The CaRe Study
RWE findings presented by Prof. Stephen Greene (Duke University School of Medicine, USA) demonstrated distinct pathways leading to combined heart failure (HF) and chronic kidney disease (CKD), including HF→CKD, CKD→HF and simultaneous presentation of both conditions. Across all pathways, substantial gaps in guideline-directed medical therapy (GDMT) utilization and limited nephrology involvement were observed. These findings highlight opportunities for earlier detection, improved multidisciplinary management and more integrated cardiorenal care.

Presented prof Stephen Greene at
ESC Heart Failure 2025
Belgrade, Serbia, May 2025.
12 FEBRUARY 2025
EHJ
Suspected de novo heart failure The REVOLUTION HF Study
This RWE study showed that patients presenting in outpatient care with suspected de novo HF—defined by new HF signs or symptoms and elevated NT-proBNP—face an immediate and very high risk of HF hospitalization and death. Risks were highest in the first weeks after presentation, underscoring the need for rapid identification, evaluation, and initiation of HF therapy.
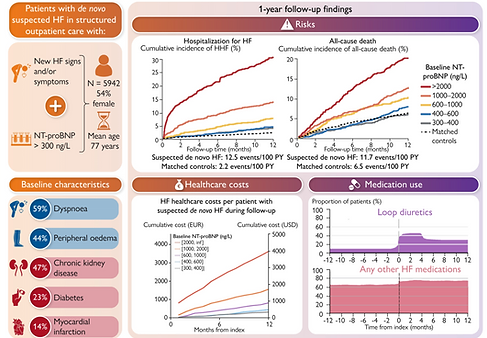
Anderson L, Bayes-Genis A, Bodegård J, Mullin K, Gustafsson S, Rosano GMC, Sundström J. Suspected de novo heart failure in outpatient care: the REVOLUTION HF study. Eur Heart J. 2025 Apr 22;46(16):1493-1503. doi: 10.1093/eurheartj/ehaf034. PMID: 39935142; PMCID: PMC12011520.